ICSI vs. conventional IVF: Which option is right for you?


With infertility rates rising, more and more couples are looking to assisted reproductive technology (ART) techniques to achieve pregnancy. The most common type by far is conventional in vitro fertilization (IVF).
In fact, according to the American Society for Reproductive Medicine, 2024 marked the first time more than 100,000 babies were born through IVF in the US within a single year, demonstrating the sheer number of families that are relying on the accessibility and advancements in fertility care nationwide.
If you as a couple have been researching and preparing for potential ART techniques, you may have come across intracytoplasmic sperm injection, or ICSI. ICSI refers to a specialized form of IVF, in which a single live sperm is injected directly into the center of an egg, unlike in IVF, when thousands of sperm and one to two eggs are mixed in a single dish so the sperm can swim and penetrate the egg(s) just as they do during natural fertilization.
During an ICSI procedure, an embryologist will select the single best sperm based on its morphology and motility to prepare for injection.1 This meticulous form of IVF was developed for couples experiencing severe male factor infertility or those who’ve experienced previous fertilization failures through conventional IVF. As a result, it’s also generally more expensive.
When determining which option is right for you — ICSI vs. IVF — it’s important to keep all this in mind as you make the best decision for you and your family. We’ll further break down the differences between IVF and ICSI below to make this process that much easier and that less stressful.
Key takeaways
- ICSI involves directly injecting a single sperm into the center of an egg, while IVF involves combining thousands of sperm and one to two eggs in a single dish for fertilization.
- Both ICSI and IVF involve fertility testing/screenings, ovarian stimulation, egg retrieval, sperm retrieval, embryo culture and transfer, and a pregnancy test.
- ICSI is recommended for male infertility because this procedure can help overcome issues such as severely low sperm count, poor sperm motility, and/or abnormal sperm morphology.
- ICSI typically adds an additional $1,000 to $3,000 to the cost of a standard IVF cycle.
Comparing IVF vs. ICSI
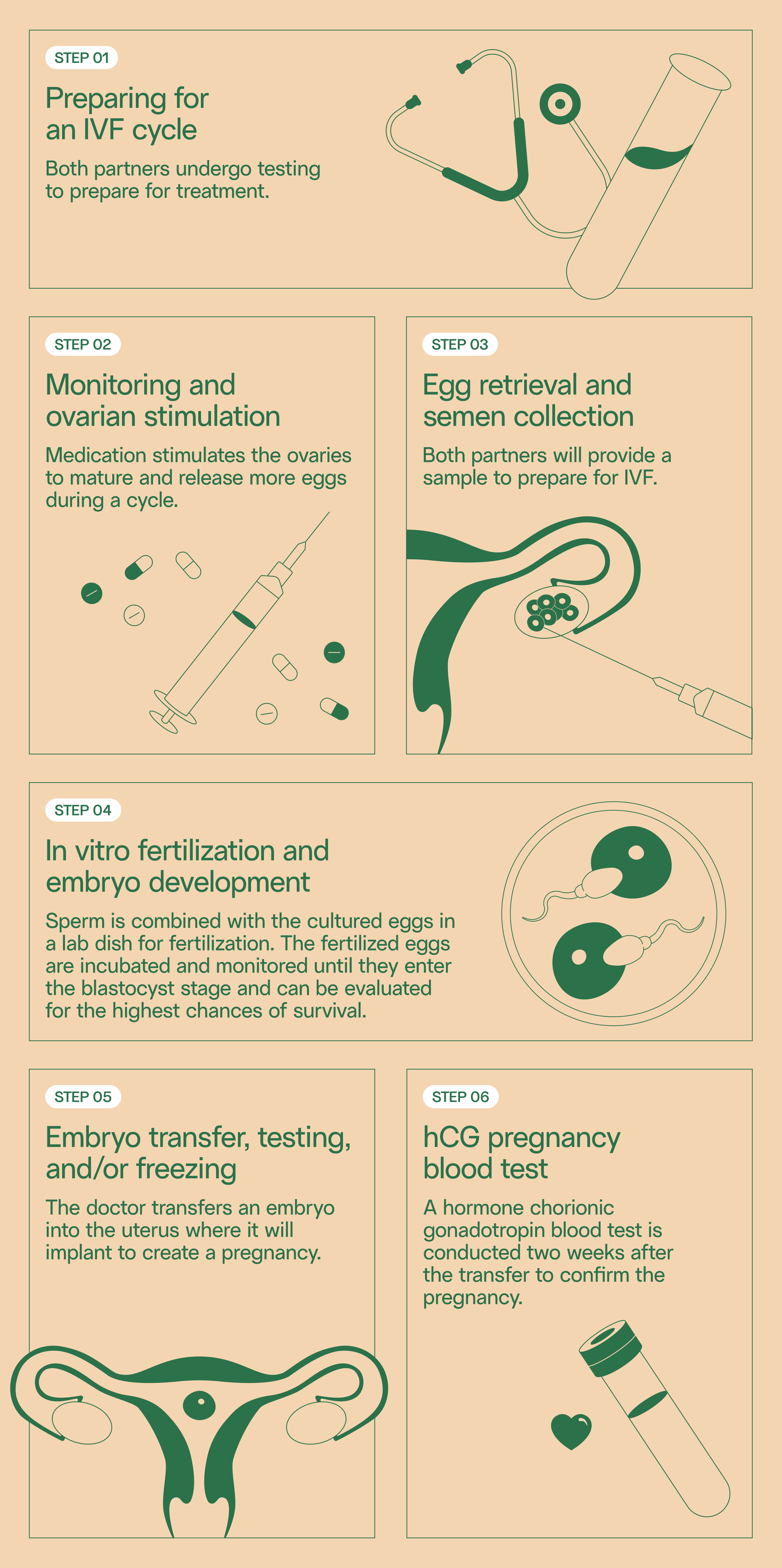
Conventional IVF step-by-step
A full IVF cycle can take an average of 4–8 weeks from start to finish, or an initial consultation to a positive pregnancy test.
Before you start a cycle of IVF, however, you and your partner will take various screening tests for your sperm and eggs, respectively. Here are some common IVF checklist items:
- Ovarian reserve testing involves blood tests to determine how many remaining eggs are in a body, based on hormone levels.
- Female hormone testing is often paired with an ultrasound to examine the ovaries and an hysteroscopy or sonohysterography to examine the inside of a uterus.
- Semen analysis involves analyzing a semen sample for concentration, count, volume, morphology, motility, and in some cases, DNA fragmentation. You can also do this from the comfort of your own home with an at-home, mail-in sperm testing kit.
- You and your partner will also test for various infectious diseases such as HIV, hepatitis, and syphilis.
- A practice embryo transfer is a painless and quick test run of the IVF embryo transfer process to determine the depth of a uterus and the best transfer technique that’s most likely to succeed.
These tests ensure you and your partner are healthy and help fertility specialists address any potential obstacles that might make it harder for you as a couple to achieve a viable pregnancy.
An IVF cycle officially begins with using lab-made hormones to stimulate the ovaries to make multiple eggs instead of the single egg that develops naturally each month. Increasing the number of eggs will increase your chances of success.
Your partner will self-administer daily injections which can contain either a follicle-stimulating hormone (FSH), a luteinizing hormone (LH), or both to help more than one egg develop at a time. Ovarian stimulation usually takes 1–2 weeks before the egg retrieval procedure. Ultrasounds of the ovaries and blood tests help determine when the eggs are ready for retrieval.
Egg retrieval is performed under general anesthesia with an ultrasound device that goes into the vagina to help the surgeon identify ovarian follicles. Then the surgeon inserts a very thin needle into the follicles to collect the eggs. The needle is connected to a gentle suction device and can remove multiple eggs in about 20 minutes. These eggs are then placed in a liquid to prepare for fertilization. This process is repeated for both ovaries.
Sperm retrieval usually occurs the morning of egg retrieval via masturbation or can be collected and frozen for safekeeping ahead of time. Sperm are retrieved and separated from semen fluid in the lab and prepped for fertilization.
During conventional IVF, thousands of healthy sperm and mature eggs are mixed together in a lab dish in hopes that the sperm will fertilize the eggs. The dish is kept in an incubator to maintain a precise, controlled, and stable environment for fertilization and embryo development.
It’s at this point where the embryologist could biopsy the embryo(s) by taking a small sample of cells, and use those cells for embryo genetic testing. Typically, the embryo(s) would then be frozen pending results.
Two to six days after the eggs have been collected (or later if you’re using a frozen embryo), a catheter attached to a syringe containing one or more embryos is inserted through the cervix and into the uterus. The surgeon uses the catheter to transfer the fertilized embryo to the uterine lining. The whole process takes about 20 minutes.
The final step of a full IVF cycle is taking a pregnancy test typically about 10 to 14 days after the embryo transfer. This will be a blood test, which is more accurate in detecting the human chorionic gonadotropin (hCG) hormone — a key marker for pregnancy — than the over-the-counter tests you’ll find in convenience stores.
Conventional IVF success rates
IVF success rates range from 5 to 55% per cycle, but are typically the highest for women under 35 at 40 to 55%. Rates steadily decline with age due to egg quantity and quality. If your partner is over 40, using donor eggs during IVF can boost your chances of success.
Other success factors that may come into play are:
- Reproductive history: If your partner has given birth before, they’re more likely to get pregnant through IVF. If your partner has tried but failed to get pregnant through IVF multiple times, your chances of success with IVF will be lower.
- Embryo status: The more developed an embryo is, the higher your chances of success. Not all embryos will survive the development process, however.
- Lifestyle factors: Smoking, obesity, and drug use can significantly lower your chances of success.
- Infertility: If your partner has severe endometriosis, your chances of pregnancy through IVF are lower than those who are experiencing female infertility problems without a clear cause. For male infertility, ICSI is a highly effective option with successful fertilization rates ranging from 70 to 80%.
To determine whether IVF might work for you before an initial consultation at a fertility clinic, you can use the online IVF Success Estimator courtesy of the CDC. This tool can estimate your chances of having a live birth through IVF once you enter some information about your background, history, reason for using IVF, and whether you plan to use your or a donor’s eggs.
ICSI step-by-step
ICSI is similar to IVF in that it also involves fertility testing/screenings, ovarian stimulation, egg retrieval, sperm retrieval, embryo culture and transfer, and a pregnancy test. The timing between these steps is comparable to that of IVF. A full cycle of ICSI also takes an average of four to eight weeks from start to finish, or initial consultation to positive pregnancy test.
The major difference is that instead of mixing thousands of sperm with mature eggs, an embryologist will use an inverted microscope and a specialized micropipette to select and immobilize a single, healthy-appearing sperm. Then, the embryologist will inject that sperm directly into the cytoplasm of a mature egg. This process is repeated for each mature egg.
ICSI success rates for couples overall range from 30 to 60% per cycle and is the highest for women under 35 at 45 to 55%.
Why is ICSI recommended for male infertility?
ICSI is recommended for male infertility because this procedure can help overcome issues such as severely low sperm count, poor sperm motility, and/or abnormal sperm morphology — all factors that can make fertilization during conventional IVF that much harder. By injecting a sperm directly into the egg, you can bypass this process entirely.
When it comes to maternal age, the ICSI success rate ranges are relatively similar to that of IVF. If you as a couple have gone through failed fertilization attempts during several IVF cycles, it's worth giving the ICSI procedure a try.
Risks of IVF and ICSI
While ICSI is considered a highly effective and safe procedure, there are still risks you should be aware of.2
Risks associated with IVF (that ICSI shares) include:
- Ovarian hyperstimulation syndrome (OHSS), or when the ovaries swell, leak fluid, and become very painful (0.1% to 2% of cycles)
- Egg retrieval complications such as infection, bleeding, or organ damage
- Multiple pregnancies
- Increased risk of preterm births or low birth weights
- Miscarriages
Risks associated with ICSI include:
- Damage to eggs during needle insertion (less than 5%)
- Potential for increased chromosomal abnormalities, particularly severe male factor infertility (about 8%)
- Slightly higher risk of developmental delays
Luckily, the risks associated with both ICSI and IVF are rare, with most patients experiencing zero complications. Still, it’s always better to be informed.
How much does IVF vs. ICSI cost?
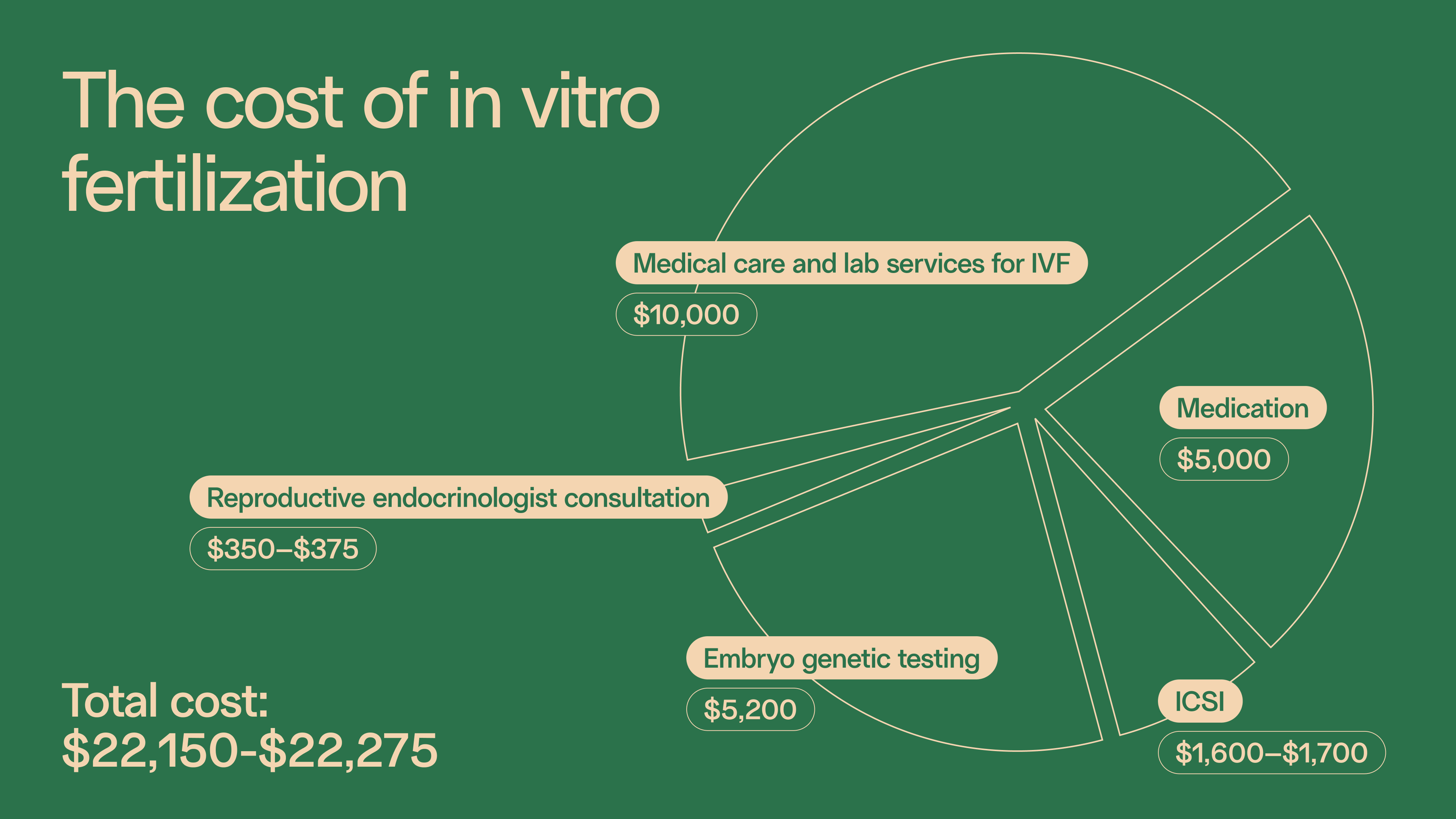
An IVF cycle can cost between $12,000 to $15,000 per cycle, but this will vary depending on many factors — namely location, maternal age, the number of cycles, any additional procedures, medications, and more.
ICSI typically adds an additional $1,000 to $3,000 to the cost of a standard IVF cycle. ICSI is more expensive because it requires more specialized equipment and skill to delicately microinject the sperm into the egg.
If your insurance covers IVF, it’s likely your plan will cover ICSI as well. ICSI is often covered if your insurance policy includes infertility benefits or if you have a male factor infertility diagnosis. Some plans may also consider ICSI as a separate, add-on service. It’s important to consult your insurance provider beforehand to determine your coverage.
Choosing what’s right for you
Ultimately, you and your partner — with the expertise of a fertility specialist — will know best in terms of what’s right for you as a couple.
IVF is often recommended for couples experiencing:
- Endometriosis and/or other uterus problems
- Blocked or damaged fallopian tubes
- Male infertility
- Polycystic ovary syndrome (PCOS)
- Unexplained infertility
IVF is also recommended for same-sex couples, couples with advanced maternal age, genetic testing needs, and single parents.
ICSI is often recommended for couples experiencing:
- Severe male factor infertility (ex: very low sperm count, poor sperm morphology and/or motility)
- Blockage in the male reproductive system
- Previous failed attempts at fertilization through conventional IVF
- The need to collect sperm surgically instead of via masturbation
- Anejaculation or the inability to ejaculate
- Retrograde ejaculation or semen entering the bladder instead of exiting the penis
ICSI is also recommended for couples using frozen eggs or frozen sperm and couples with advanced maternal age.
Taking all this into consideration will ensure you make the most informed and best decision you can together for the sake of your family.
Frequently asked questions
1. What’s the difference between IVF and ICSI?
The major difference between IVF and ICSI is that IVF mixes thousands of sperm with mature eggs (one to two) in a dish so that the sperm can swim and penetrate the egg(s) just as they do during natural fertilization, while ICSI involves an embryologist using an inverted microscope and specialized micropipette to select and immobilize a single, healthy sperm to then inject directly into the cytoplasm of a mature egg.
2. Can IVF fail if sperm quality is low?
Yes, IVF can fail if sperm quality is low because severely low sperm count, poor sperm motility, and/or abnormal sperm morphology can make fertilization during conventional IVF that much harder as well as lead to poor embryo development and increased risk of miscarriage.
Learn more about sperm quality's impact on embryo quality.
3. Is ICSI more expensive than IVF?
Yes, ICSI is more expensive than IVF because it requires more specialized equipment and skill to delicately microinject the sperm into the egg.
4. Are there higher risks with ICSI?
Yes, though rare, there are slightly higher risks with ICSI than IVF because of potential damage to the egg due to needle insertion and because bypassing the natural fertilization process can increase the risk of genetic issues being passed down.
5. Can IVF and ICSI be combined?
Yes, ICSI in conjunction with IVF is an option for couples and might be especially promising for those with a history of poor fertilization.
References
When it comes to getting pregnant, sperm is half the equation.


Advanced Semen Analysis with DNA Fragmentation Testing
$495
Key features

Semen volume
Sperm concentration & count
Motility
Morphology
Sperm DNA fragmentation



